
Protective Actions and Protective Action Guides
- EPA
- Protective Actions
- Protective Action Guides (PAGs)
- Exposure Pathways and Protective Actions: Chart
- Summary Table for PAGs, Guidelines, and Planning Guidance for Radiological Incidents by Phase of Incident
- PAGS and Protective Actions for the Early Phase of a Radiological Incident
- EPA Emergency Worker Exposure Guidelines
- Protective Action Guidance for Food and Drinking Water
- Generalized Protective Action Areas for Nuclear Power Plant Incident
- Protective Action Guides for Exposure to Deposited Radioactivity during the "Intermediate Phase" of a Radiological Incident
- Reentry Matrix Following a Radiation Incident or Accident by Phase of Incident
- Other Agencies' Radiation Protection Recommendations
Protective Actions
-
Protective actions (protective action recommendations): designed to be taken before an anticipated Protective Action Guide (PAG) dose is reached.
-
Actions taken to reduce or eliminate the public's exposure to radiation or other hazards following an radiation incident
- In the early and intermediate phases of RDD/IND incidents there may be inadequate information to determine precisely the radiation levels or make dose projections.
- Initial protective actions may be undertaken based on models rather than actual measured radiation levels.
- Protective action recommendations may change over the course of an incident, as new information is obtained.
-
Primary protective actions include
- Sheltering-in-place
- Evacuation
- Relocation
- Interdiction of food and water
-
Secondary protective actions include
- Medical countermeasure administration
- Decontamination of people and places
- Restrictions of food and/or water
- Access control
- Victim extraction
-
See also:
- Definitions in REMM dictionary for additional details
-
Actions taken to reduce or eliminate the public's exposure to radiation or other hazards following an radiation incident
Protective Action Guides (PAGs)
- Key federal PAG guidance description and documents
- PAG Manual: Protective Action Guides and Planning Guidance for Radiological Incidents, EPA-400/R-17/001 (PDF - 1.48 MB) (EPA, January 2017)
- Protective Action Area Map Templates (download as word document (10 pp, 16 MB, September 2017, EPA-420/K-17/003)
- Templates for state, local, and tribal governments that need to provide evacuation, go inside, food, and/or drinking water guidance quickly to a population in a specific geographical area
- Protective Action Questions and Answers for Radiological and Nuclear emergencies: A companion document to the US EPA PAG Manual (PDF - 3.51 MB) (EPA, September 2017)
- Communicating Radiation Risks: Crisis Communications for Emergency Responders (PDF - 18.2 MB) (EPA, September 2007)
- Federal Register announcement about the EPA Radiation PAG Manual (December 1, 2016)
- PAG notice at Regulations.gov
- PAG Manual Fact Sheet (PDF - 275 KB) (December 2016)
- EPA library of current and former radiation PAG Manuals and Resources
- Federal Register Announcement about Revision to the PAG Manual: Protective Action Guide (PAG) for Drinking Water after a Radiological Incident (EPA, 1/2017)
- Chapter 4, Section 4.6, pages 53-68 of the 2017 PAG Manual incorporates guidance for radiation protection guidance on drinking water.
- See REMM page for more details on Monitoring Radionuclides in Drinking Water and Food: Routinely and After a Release
- General concepts about PAGs from page 1 of the 2017 Manual
- PAGs are guides to help officials select protective actions under emergency conditions during which exposures would occur for relatively short time periods.
- They are not meant to be applied as strict numeric criteria, but rather as guidelines to be considered in the context of incident specific factors.
- PAGs do not establish an acceptable level of risk for normal, non-emergency conditions, nor do they represent the boundary between safe and unsafe conditions.
- The PAGs are not legally binding regulations or standards and do not supersede any environmental laws.
- Protective Action Area Map Templates (download as word document (10 pp, 16 MB, September 2017, EPA-420/K-17/003)
- Description of Protective Action Guides (PAGs)
- PAG Manual: Protective Action Guides and Planning Guidance for Radiological Incidents, EPA-400/R-17/001 (PDF - 1.48 MB) (EPA, January 2017)
- Additional emergency response PAG guidance
- The Department of Homeland Security/ Federal Emergency Management Agency
- Planning Guidance for Protection and Recovery Following Radiological Dispersal Device (RDD) and Improvised Nuclear Device (IND) Incidents (2008) This provides an interim supplement to the 1992 document cited above.
- The Homeland Security Council
- Planning Guidance for Response to a Nuclear Detonation, Second Edition (PDF - 2.47 MB) (June, 2010)
- Department of Energy
- Federal Radiological Monitoring and Assessment (FRMAC, April 2015), FRMAC Assessment Manual, Volume 1 - Overview and Methods (PDF - 2.66 MB)
- Federal Radiological Monitoring and Assessment (FRMAC, February 2010), FRMAC Assessment Manual, Volume 2 - Pre-assessed Default Scenarios (PDF - 3.94 MB)
- Food and Drug Administration
- Guidance: Potassium Iodide as a Thyroid Blocking Agent in Radiation Emergencies, December, 2001 (PDF - 40 KB)
- Guidance for Industry KI in Radiation Emergencies -Questions and Answers, December 2002 (PDF - 161 KB)
- Frequently Asked Questions about KI
- Food and Drug Administration: Accidental Radioactive Contamination of Human Food And Animal Feeds: Recommendations for State and Local agencies (PDF - 231 KB) (1998)
- Centers for Disease Control and Prevention
- NCRP
- Responding to a Radiological or Nuclear Terrorism Incident: A Guide for Decision Makers (PDF - 1.61 MB) (NCRP Report No. 165), Bethesda, MD, 2010.
- The Department of Homeland Security/ Federal Emergency Management Agency
Exposure Pathways and Protective Actions: Chart
Potential Exposure Pathways and Protective Actions by Incident Phase
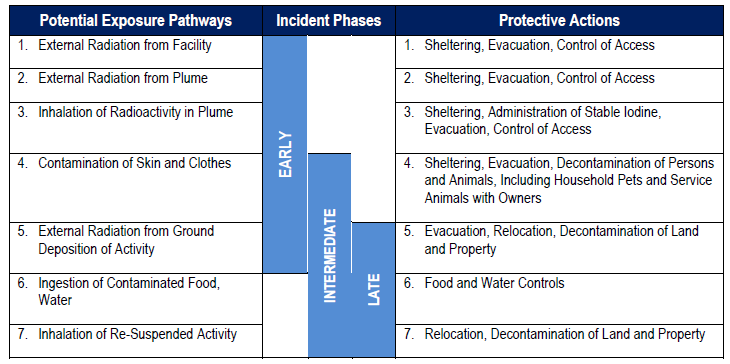
Source: Nuclear/Radiological Incident Annex to the Response and Recovery Federal Interagency Operational Plans, (PDF - 3.38 MB) (US Government Interagency, October 2016, See Figure 3, page 46)
- Early Phase (Aligns to operational Phase 2a):
- The Early Phase is the period at the beginning of the incident when immediate decisions for effective protective actions are required.
- There may be little or no information available on actual releases or field measurement data.
- Protective actions in the early phase are aimed at avoiding inhalation of gases or particulates in a plume and minimizing external exposure.
- Intermediate Phase (Aligns to operational Phases 2a, 2b, and 2c):
- The Intermediate Phase may overlap with and/or follow the early phase response within as little as a few hours and can last for weeks or months.
- This phase is assumed to begin after the incident source and releases have been brought under control and protective action decisions can be made based on measurements of exposure and radioactive materials that have been deposited.
- Protective actions in the intermediate phase are intended to reduce or avoid dose to the public, control worker exposures and the spread of contamination, and prepare for late-phase cleanup.
- Late Phase (Aligns to operational Phase 2c and 3):
- The Late Phase is the period when actions designed to reduce radiation levels in the environment to acceptable levels are conducted.
- The late phase entails final clean-up decisions and implementation of remediation strategies.
- The Late Phase will overlap with the intermediate phase response, making Phase 2c part of both the intermediate and late phases.
Summary Table for PAGs, Guidelines, and Planning Guidance for Radiological Incidents by Phase of Incident
(Source: EPA PAG Manual 2017 (PDF - 1.48 MB), See Table 1-1, page 6)
Summary Table for PAGs, Guidelines, and Planning Guidance for Radiological Incidentsa
| Phase | Protective Action Recommendation | PAG, Guideline or Planning Guidance |
|---|---|---|
| Early Phase | Sheltering-in-place or evacuation of the publicb | PAG: 1 to 5 rem (10 mSv to 50 mSv) projected dose over four daysc |
| Supplementary administration of prophylactic drugs KId | PAG: 5 rem (50 mSv) projected child thyroid dosee from exposure to radioactive iodine | |
| Limit emergency worker exposure (total dose incurred over entire response) | Guideline: 5 rem (50 mSv)/year (or greater under exceptional circumstances)f | |
| Intermediate Phase | Relocation of the public | PAG: ≥ 2 rem (20 mSv) projected dosec in the first year, 0.5 rem (5 mSv)/year projected dose in the second and subsequent years |
| Apply simple dose reduction techniques | Guideline: < 2 rem (20 mSv) projected dose c in the first year | |
| Food interdictiong | PAG: 0.5 rem (5 mSv)/year projected whole body dose, or 5 rem (50 mSv)/year to any individual organ or tissue, whichever is limiting | |
| Drinking water | PAG: 100 mrem (1 mSv or 0.1 rem) projected dose, for one year, to the most sensitive populations (e.g., infants, children, pregnant women and nursing women); 500 mrem (5 mSv or 0.5 rem) projected dose, for one year, to the general population |
|
| Limit emergency worker exposure (total dose incurred over entire response) | Guideline: 5 rem (50 mSv)/year | |
| Reentry | Guideline: Operational Guidelinesh (stay times and concentrations) for specific reentry activities (See Section 4.6) | |
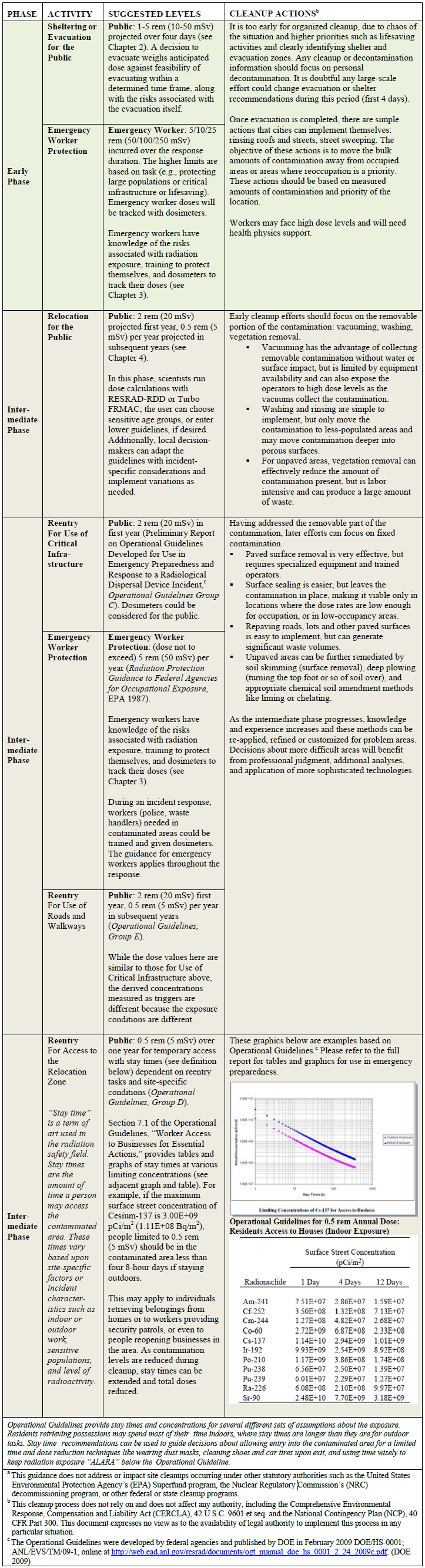
| Late Phase | Cleanup i | Planning Guidance: Brief description of planning process (see Section 5.1) |
| Waste Disposal | Planning Guidance: Brief description of planning process (see Section 5.2) | |
|
a
This guidance does not address or impact site cleanups occurring under other statutory authorities such as the United States Environmental Protection Agency’s (EPA) Superfund program, the Nuclear Regulatory Commission’s (NRC) decommissioning program, or other federal or state cleanup programs. b Should begin at 1 rem (10 mSv); take whichever action (or combination of actions) that results in the lowest exposure for the majority of the population. Sheltering may begin at lower levels if advantageous. c Projected dose is the sum of the effective dose from external radiation exposure (e.g., groundshine and plume submersion) and the committed effective dose from inhaled radioactive material. d Provides thyroid protection from radioactive iodines only. See the complete 2001 FDA guidance, "Potassium Iodide as a Thyroid Blocking Agent in Radiation Emergencies." Further information is also available in “KI in Radiation Emergencies, 2001 – Questions and Answers” 2002, and “Frequently Asked Questions on Potassium Iodide (KI).” e Thyroid dose. See Section 1.4.2. For information on radiological prophylactics and treatment other than KI, refer to http://www.fda.gov/Drugs/EmergencyPreparedness/BioterrorismandDrugPreparedness/ucm063807.htm, https://www.emergency.cdc.gov/radiation, and www.orau.gov/reacts. f When radiation control options are not available, or, due to the magnitude of the incident, are not sufficient, doses to emergency workers above 5 rem (50 mSv) may be unavoidable and are generally approved by competent authority. For further discussion see Chapter 3, Section 3.1.2. Each emergency worker should be fully informed of the risks of exposure they may experience and trained, to the extent feasible, on actions to be taken. Each emergency worker should make an informed decision as to how much radiation risk they are willing to accept to save lives. g For more information on food and animal feeds guidance, the complete FDA guidance may be found at http://www.fda.gov/downloads/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/UCM094513.pdf. h For extensive technical and practical implementation information please see "Preliminary Report on Operational Guidelines Developed for Use in Emergency Preparedness and Response to a Radiological Dispersal Device Incident" (DOE 2009). i This cleanup process does not rely on and does not affect any authority, including the Comprehensive Environmental Response, Compensation and Liability Act (CERCLA), 42 U.S.C. 9601 et seq. and the National Contingency Plan (NCP), 40 CFR Part 300. This document expresses no view as to the availability of legal authority to implement this process in any particular situation. |
||
(Source: EPA PAG Manual 2017 (PDF - 1.48 MB), See Table 1-1, page 6)
- See more detailed guidance in the EPA PAG Manual for
- PAGs and Protective Actions for the Early Phase of Radiological Incident (page 16)
- PAGs and Protective Actions for the Intermediate Phase of Radiological Incident (page 42)
- Reentry matrix: Quick Reference to Operational Guidelines (page 50) and below on this page.
- See REMM page on Phases of a radiation incident
PAGs and Protective Actions for the Early Phase of a Radiological Incident
PAGS and Protective Actions for the Early Phase of a Radiological Incidenta
| Protective Action Recommendation | PAG | Comments |
|---|---|---|
| Sheltering-in-place or evacuation of the publicb | PAG: 1 to 5 rem (10 mSv to 50 mSv) projected dose over four daysc | Evacuation (or, for some situations, sheltering-in-place) should be initiated when projected dose is 1 rem (10 mSv). |
| Supplementary administration of prophylactic drugs - KId | PAG: 5 rem (50 mSv) projected child thyroid dosee from exposure to radioactive iodine | KI is most effective if taken prior to exposure. May require approval of state medical officials (or in accordance with established emergency plans). |
|
a This guidance does not address or impact site cleanups occurring under other statutory authorities such as the United States Environmental Protection Agency’s (EPA) Superfund program, the Nuclear Regulatory Commission’s (NRC) decommissioning program, or other federal or state cleanup programs. b Should begin at 1 rem (10 mSv) if advantageous except when practical or safety considerations warrant using 5 rem (50 mSv); take whichever action (or combination of actions) that results in the lowest exposure for the majority of the population. Sheltering may begin at lower levels if advantageous. c Projected dose is the sum of the effective dose from external radiation exposure (e.g., groundshine and plume submersion) and the committed effective dose from inhaled radioactive material. d Provides thyroid protection from radioactive iodines only. The complete FDA guidance may be found at http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm080542.pdf. Further information is also available: http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm080546.pdf and http://www.fda.gov/Drugs/EmergencyPreparedness/BioterrorismandDrugPreparedness/ucm072265.htm. e Thyroid dose. For information on radiological prophylactics and treatment other than KI, refer to http://www.fda.gov/Drugs/EmergencyPreparedness/BioterrorismandDrugPreparedness/ucm063807.htm, https://www.emergency.cdc.gov/radiation, and www.orau.gov/reacts. The one-year old age group is expected to receive the largest dose to the thyroid from exposure to radioactive iodine. Therefore, it is recommended that the one-year old age group is considered when considering the administration of prophylactic KI. | ||
(Source: EPA PAG Manual 2017 (PDF - 1.48 MB), See Table 2-1, page 16)
- See PAG Manual for detailed guidance about the Early Phase of an Incident
EPA Emergency Worker Exposure Guidelines
(Source: EPA PAG Manual 2017 (PDF - 1.48 MB), See Table 3-1, page 35)
(Bullets below are from the Manual)
- Emergency worker guidelines are based on cumulative dose constraint levels incurred over the duration of an emergency and are assumed to be “once in a lifetime” doses and that future radiological exposures would be substantially lower
- Recommendations in this Manual provide a guideline level of 5 rem (50 mSv) for worker protection and alternative emergency worker guidelines (see Table 3-1) for certain activities where doses above 5 rem (50 mSv) cannot be avoided.
- For most radiological incidents, radiation control measures (e.g., minimizing time, maximizing distance, using shielding) will prevent doses from reaching the 5 rem (50 mSv) occupational exposure guideline while performing typical emergency response activities such as transportation, firefighting and medical treatment of contaminated victims at hospitals.
- However, in those situations in which victims are injured or trapped in high radiation areas or can only be reached via high radiation areas, or for protection of critical infrastructure, exposure control options may be unavailable or insufficient and doses above 5 rem (50 mSv) may be unavoidable.
- Decisions to take response actions that could result in doses in excess of 5 rem (50 mSv) can only be made at the time of the incident, under consideration of the actual situation.
- In such situations, incident commanders and other responders need to understand the risk posed by such exposures in order to make informed decisions.
- The emergency worker guidelines for life and property saving activities in Table 3-1 are provided to assist such decision-making.
- These guidelines apply to doses incurred over the duration of an emergency and are assumed to be once in a lifetime.
- After the early phase, it is likely that no more lifesaving missions would be needed.
- However, some critical infrastructure/key resources or lifesaving missions may arise in the intermediate phase, where these guidelines would apply.
- Emergency personnel may be exposed to increased radiation during the unique catastrophic event of an IND detonation resulting in firestorm and widespread destruction of structures.
- The emergency intervention needed to prevent further destruction and loss of life may result in increased exposure.
- Exceeding the emergency worker guidelines in Table 3-1 may be unavoidable in responding to such events.
- For all exposures, emergency workers must be fully informed of the risks of exposure they may experience, including numerical estimates of the risk of delayed health effects, and must be trained, to the extent feasible, on actions to be taken.
- Each emergency worker should make an informed decision as to how much radiation risk they are willing to accept to complete a particular mission.
- The 25 rem (250 mSv) lifesaving emergency worker guidelines provide assurance that exposures will not result in detrimental deterministic health effects (i.e., prompt or acute effects).
- However, it could increase the risk of stochastic (chronic) effects, such as the risk of cancer.
- Response actions that could cause exposures in excess of the 25 rem (250 mSv) emergency worker guideline should only be undertaken with an understanding of the potential acute effects of radiation to the exposed responder (see Table 3-2) and only when the benefits of the action (i.e., lifesaving or critical infrastructure/key resource protection) clearly exceed the associated risks.
- See PAG document for important additional details.
Guideline |
Worker Activity |
Condition |
|---|---|---|
5 rem (50 mSv) |
All occupational exposures |
|
10 rem (100 mSv)a |
Protecting critical infrastructure necessary for public welfare (e.g., a power plant) |
|
25 rem (250 mSv)b |
Lifesaving or protection of large populations |
|
>25 rem (250 mSv) |
Lifesaving or protection of large populations |
|
a For potential doses >5 rem (50 mSv), medical monitoring programs should be considered.
b In the case of a very large incident, such as an IND, incident commanders may need to consider raising the property and lifesaving emergency worker guidelines to prevent further loss of life and massive spread of destruction.
NCRP recommends, when the cumulative absorbed dose to an emergency responder reaches 50 rad (0.5 Gy), a decision be made on whether or not to withdraw the emergency responder from the Hot Zone (>10 mR/h = >0.1 mSv/h. NCRP considers the 50 rad (0.5 Gy) cumulative absorbed dose a decision dose, not a dose limit. (Source: Responding to a radiological or nuclear terrorism incident: a guide for decision makers. Bethesda, MD: NCRP. Report No. 165, 2011)
This guidance does not address or impact site cleanups occurring under other statutory authorities such as the United States Environmental Protection Agency’s (EPA) Superfund program, the Nuclear Regulatory Commission’s (NRC) decommissioning program, or other federal or state cleanup programs.
Protective Action Guidance for Food and Drinking Water
- The EPA PAG Manual 2017, (Section 4.6, pages 53-68), contain extensive guidance on this topic.
- See REMM page for more details on Monitoring Radionuclides in Drinking Water and Food: Routinely and After a Release
- The bullets below are quoted from the EPA PAG Manual 2017 document
- EPA developed a new drinking water PAG as non-regulatory guidance to protect the public in the event of a radiological incident that affects drinking water supplies.
- The purpose of the protective action for the drinking water exposure pathway is to restrict the use of contaminated water for drinking and to provide recommendations for local communities to consider in providing alternative drinking water for the affected community during a nationally significant radiological incident, such as a disaster at a nuclear power plant, an RDD or an IND.
- The drinking water PAGs apply during the intermediate phase of an incident, which may last for weeks to months but not longer than one year.
- This guidance only provides recommendations and does not confer any legal rights or impose any legally binding requirements upon any member of the public, states, or any other federal agency.
- The drinking water PAG will help federal, state, local and public water system officials make decisions about use of water during radiological emergencies.
- The drinking water PAG is for use only during an emergency; it is not a substitute for compliance with EPA’s National Primary Drinking Water Regulations (NPDWRs) for Radionuclides. EPA expects that any drinking water system adversely impacted during a radiation incident will take action to return to compliance as soon as possible
- The PAG includes both EPA guidance and other standards as wells as guidance about how to interpret and apply the PAG guidance
- Drinking water guidance in the PAG manual discusses the following
- Safe Drinking Water Act (SDWA) (EPA)
- Derived Response Levels (DRLs) for radionuclides likely to appear in drinking water following a radiological contamination incident.
- Maximum contaminant level (MCL) for radionuclides in water
- Information from Public Health England about Drinking Water Supplies (PHE, 2015)
- Information from Public Health England about Food Production Systems (PHE, 2015)
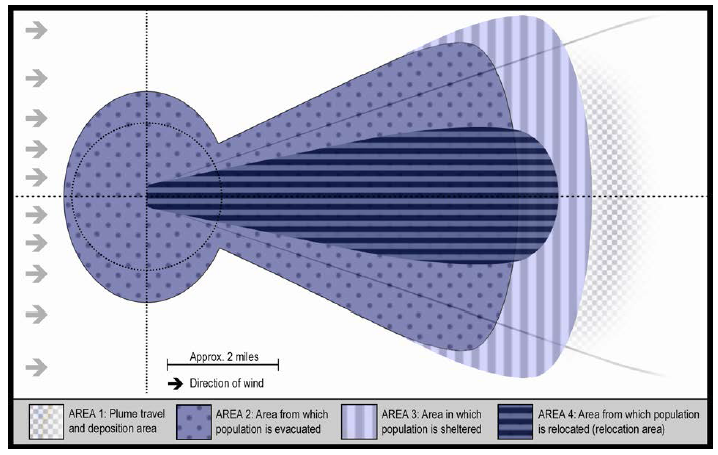
Generalized Protective Action Areas for Nuclear Power Plant Incident
(Source: EPA PAG Manual 2017 (PDF - 1.48 MB), See Figure 4-1, page 54. See also entire PAG Manual section on Intermediate Phase: Relocation and Dose Reduction)
(Source: EPA PAG Manual 2017 (PDF - 1.48 MB), See Figure 4-1, page 54. See also entire PAG Manual section on Intermediate Phase: Relocation and Dose Reduction)
Protective Action Guides for Exposure to Deposited Radioactivity during the "Intermediate Phase" of a Radiological Incident
(Source: EPA PAG Manual 2017 (PDF - 1.48 MB), See Table 4-1, page 42)
PAGs and Protective Actions for Exposure to Deposited Radioactivity during the Intermediate Phase of a Radiological Incidenta
| PAG or Guideline | Comments | |
|---|---|---|
| Relocation of the publicb |
PAG:
≥ 2 rem (20 mSv) projected dosec in the first year, 0.5 rem (5 mSv)/year projected dosec in the second and subsequent years |
Projected dose over one year of exposure. |
| Apply simple dose reduction techniquesd | Guideline: < 2 rem (20 mSv) projected dosec in the first year | These protective actions should be taken to reduce doses to as low as practicable levels |
| Food interdictione | PAG: 0.5 rem (5 mSv)/year projected whole body dose, or 5 rem (50 mSv)/year to any individual organ or tissue, whichever is limiting | |
| Drinking Water |
PAG: 100 mrem (1 mSv or 0.1 rem) projected dose, for one year, to the most sensitive populations (e.g., infants, children, pregnant women and nursing women); 500 mrem (5 mSv or 0.5 rem) projected dose, for one year, to the general population |
See Section 4.6 |
| Reentry | Guideline: Operational Guidelinesf (stay times and concentrations) for specific reentry activities (see Section 4.6) | |
|
a This guidance does not address or impact site cleanups occurring under other statutory authorities such as the United States Environmental Protection Agency’s (EPA) Superfund program, the Nuclear Regulatory Commission’s (NRC) decommissioning program, or other federal or state cleanup programs. b People previously evacuated from areas outside the relocation area defined by this PAG may return to occupy their residences. Cases involving relocation of people at high risk from such action (e.g., patients under intensive care) may be evaluated individually. c Projected dose refers to the dose that would be received, by default, in the absence of shielding from structures or the application of dose reduction techniques. These PAGs may not provide adequate protection from some long-lived radionuclides (see Section 4.5). Incident-specific factors should be considered. d Simple dose reduction techniques include scrubbing or flushing hard surfaces, minor removal of soil from spots where radioactive materials have concentrated, and spending more time than usual indoors or in other low exposure rate areas. e For more information on food and animal feeds guidance, the complete FDA guidance may be found at http://www.fda.gov/downloads/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/UCM094513.pdf. f For extensive technical and practical implementation information please see "Preliminary Report on Operational Guidelines Developed for Use in Emergency Preparedness and Response to a Radiological Dispersal Device Incident" (DOE 2009). |
||
Reentry Matrix Following a Radiation Incident or Accident by Phase of Incident
(Source: EPA PAG Manual 2017 (PDF - 1.48 MB), See Table 4-2, page 50-52)
Worker Protection Recommendations from Professional Societies
Agency |
Summary Information |
Original Document |
|---|---|---|
National Council on Radiation Protection and Measurements (NCRP) |
Recommendations for Emergency Responders |
Responding to a Radiological or Nuclear Terrorism Incident: A Guide for Decision Makers (PDF - 1.61 MB) (NCRP Report No. 165, Section 3.2.1 and 3.2.2), Bethesda, MD, 2010. |
National Council on Radiation Protection and Measurements (NCRP) |
NCRP Radiation Protection Guidelines: Control of Radiation Dose in the Control Zones |
Key Elements of Preparing Emergency Responders for Nuclear and Radiological Terrorism (NCRP Commentary No. 19), National Council on Radiation Protection and Measurements, Bethesda, MD, December 2005, page 19. Purchase required. |
International Atomic Energy Agency (IAEA) |
Manual for First Responders to a Radiological Emergency (PDF - 2.2 MB) (CTIF, IAEA, PAHO, WHO, October 2006, page 41) |
|
International Atomic Energy Agency (IAEA) |
Updated guidance based on exercises and actual incidents with comprehensive safety standards for protecting people and the environment. |
Preparedness and Response for a Nuclear or Radiological Emergency, IAEA Safety Standards Series GSR part 7, 2015 (Jointly sponsored by IAEA and 12 other organizations noted on cover page) |
Conference of Radiation Control Program Directors, Inc. (CRCPD) |
Handbook for Responding to a Radiological Dispersal Device (Dirty Bomb): First Responder's Guide: The First 12 Hours (CRCPD Publication 06-6) (page 28) Conference of Radiation Control Program Directors, Inc. Frankfort, Kentucky, 2006. |
|
International Commission on Radiological Protection (ICRP) |
Protecting People Against Radiation Exposure in the Event of a Radiological Attack (ICRP Publication 96), International Commission on Radiological Protection, 2005, page 51. |
See also: Personal Protective Equipment (PPE)
Reference Values for Emergency Responder Radiation Safety
Terminology |
Accumulated Dose |
Recommended Application or Action |
Document |
|---|---|---|---|
Response worker guidelines |
5 rem |
All occupational exposures |
PAG Manual: Protective Action Guides and Planning Guidance for Radiological Incidents (EPA, 2017) |
Decision dose |
50 rad |
Decide whether to remove responder or continue mission, based on operational awareness and mission priorities |
|
Turn-back dose guidance |
50 rem |
Prevent severe health effects or injuries |
Manual for First Responders to a Radiological Emergency (IAEA, 2006) |
Cold zone |
≤0.01 R h-1 |
Alarm threshold |
Key Elements of Preparing Emergency Responders for Nuclear or Radiological Terrorism (NCRP, 2005) |
Hot zone |
>0.01 R h-1 |
Routine response activities performed with personal protective equipment, including active radiation monitoring |
Key Elements of Preparing Emergency Responders for Nuclear or Radiological Terrorism (NCRP, 2005) |
Dangerous-radiation zone |
≥10 R h-1 |
Restrict actions to time sensitive, mission critical such as lifesaving |
|
Turn back |
200 R h-1 |
Responders should turn back, even when working on life saving missions |
Note: Local agencies may have alternate guideline values for responder operations.
Source: Guidance for Emergency Response Dosimetry (NCRP Report 179), National Council on Radiation Protection and Measurements, Bethesda, MD, 2017, Table 4.1.
Regulations for Worker Protection: US Government Agencies
- The Occupational Safety and Health Act requires employers to be responsible for the health and safety of their employees during routine and emergency operations. OSHA guidance may not be fully applicable in a large emergency when workers who are not trained as "radiation workers" are added to the response force.
- This is a very complex topic.
- The EPA PAG Manual 2017 (PDF - 1.48 MB), in Table 3-3, page 38, shown below, provides more detailed guidance than is provided on REMM.
Regulations for Worker Protection
| Agency | Statutory Requirement | Title |
|---|---|---|
| Occupational Safety and Health Administrationa | 29 CFR 1910.120 | Safety and Health-- HAZWOPER |
| 29 CFR 1910.1096 | Ionizing Radiation | |
| Environmental Protection Agencya | 40 CFR 311 | Occupational Radiation Protection |
| Nuclear Regulatory Commissionb | 10 CFR 20 | Standards for Protection Against Radiation |
| Department of Energyc | 10 CFR 835 | Radiation Protection Regulations |
|
a Worker safety and health is regulated in all states by federal OSHA or by respective state regulations under an OSHA-approved state plan. 40 CFR Part 311 applies the OSHA HAZWOPER standard (29 CFR 1910.120) to public-sector workers in states that do not operate their own occupational safety and health programs. b It is the NRC’s position (56 FR 23365) that dose limits for normal operations should remain the primary guideline in emergencies to the extent practicable. However, in accordance with 10 CFR 20.1001(b), conformance with such dose limits should not hinder an NRC licensee from taking actions that may be necessary to protect public health and safety in an emergency. c These requirements apply to all DOE employees and contractors (except for Naval Nuclear Propulsion Program (NNPP)) who may be exposed to ionizing radiation as a result of their work for DOE, including work relating to emergency response activities. The NNPP has established requirements consistent with those contained in 10 CFR Part 835. | ||