
Fallout from a Nuclear Detonation:
Description and
Management
- Source of This Guidance
- Intended Audience for This Guidance
- Key Points
- Understanding Fallout
- Population Monitoring and Decontamination
- Key Points from Other Important Documents
- Key Quotes from Other Important Documents
Sources of This Guidance
-
Buddemeier BR,
Nuclear Detonation Fallout: Key Considerations for
Internal Exposure and Population Monitoring
(DOE/LLNL
LLNL-TR-754319 , July 6, 2019) - This REMM page quotes extensively from text in this monograph and presents many of its excellent graphics.
Intended Audience for This Guidance
- Regional, state and local responders who have responsibility for developing local IND response plans
- Medical and public health responders
Key Points
- Contamination with radioactive fallout is NOT immediately life-threatening to the population or the responders who assist them. This is unlike many chemical and biological events.
-
The primary radiation hazard from fallout after a nuclear
detonation arises from
external exposure
to penetrating radiation released from the decaying
radioactive particles, rather than from
internal contamination (exposure)
from
breathing
or
ingesting
radioactive material.
- External radiation exposure from fallout represents the greatest preventable injury after a nuclear detonation.
-
The earliest priority of any population
monitoring activity is identification and care of
individuals whose health is in immediate danger (from trauma
or serious medical disorders) and who require urgent care.
- This activity takes precedence over detailed radiological assessment for external or internal contamination and complex detection and decontamination procedures, especially early on in the incident.
- Urgent medical treatment for life-threatening conditions should never be delayed due to contamination concerns.
- Shelter should never be denied due to contamination concerns.
- AFTER providing urgent care, the next priority for population monitoring, in the early period following a nuclear detonation, is detection and removal of external contamination for those whose prior location (e.g. Dangerous Fallout Zone) suggests they were at greatest risk. Assessing dose from exposure is also important, but it is not the subject of this monograph.
-
In most cases, external decontamination can be
self-performed, especially early on when resources (radiation survey
equipment, personnel and space) are constrained.
- Straightforward instructions about decontamination must be provided, “Improvised Nuclear Device Response and Recovery Communicating in the Immediate Aftermath” (PDF - 1.11 MB) (DHS/FEMA, June 2013)
- Fallout is likely to be large salt and sand-sized particles, like dirt, that can be easily removed with brushing and gentle wiping.
- Initially, simple self-decontamination (e.g., brushing off clothes and skin) is recommended, even if precise levels of external contamination have not been measured and documented with radiation monitoring equipment and no showering or clothing/shoe replacement is feasible.
-
Radiation monitoring equipment and response resources
(e.g., staff and space) will be critically limited in the
initial days after a detonation.
- Initially, radiation monitoring equipment should be used for responder safety, hazard mapping, and search and rescue activities.
- Mass decontamination (i.e. fire hose wash down) techniques used in colder climates can result in more casualties from hypothermia than would have occurred from contamination.
Understanding Fallout
Basic Information
- There will be large numbers of people, perhaps over a million, from fallout contaminated areas who may have some level of detectable contamination (e.g., after a 10 kT detonation). See REMM page about designations of Fallout Zones and fallout changes over time.
- Fallout contamination decays rapidly (giving off > 80% of its energy in the first day (see Figure 2 on this page), so early, gross decontamination (such as removing or changing outer layer of clothing) is far more effective than a delayed, if more thorough, wash down.
- A nuclear explosion, especially a ground burst, can produce fallout, which is generated when dust and debris created by the explosion are combined with radioactive fission products and drawn upward into the cloud produced by the detonation.
- Due to the heat of the explosion, the cloud rapidly climbs through the atmosphere, potentially reaching heights of 5 miles (8 km) for a 10-kiloton explosion. Under ideal conditions it would form a mushroom-shaped cloud.
- Highly radioactive particles drop back down to earth as the cloud cools. When it reaches ground and covers the surface of buildings, it is also called “groundshine”.
- Larger particles tend to fall closer to the detonation site, whereas small particles, such as those that might pose an inhalation hazard, tend to stay in the upper atmosphere much longer, perhaps for days or weeks.
- Although details about how far fallout travels are highly dependent on weather conditions, the most dangerous concentrations of fallout particles (i.e., potentially fatal external exposures to those outdoors) occur within 10 to 20 miles downwind of the explosion (from a 10 kT detonation). The perimeter of the fallout zones will change rapidly over time as the radionuclides decay.
- Fallout particles are clearly visible as they fall, often being the size of fine sand or table salt. (NCRP, Symposium Proceedings1982).
- Rain or “washing of fallout areas” might concentrate fallout in sewers and storm drains, but such action would be accompanied by a reduction of fallout concentration elsewhere.
- Dangerous levels of fallout can create visible dust and debris, so visible fallout can be used as an indicator of a direct radiation hazard. However, fallout might not be readily noticeable on rough or dirty surfaces after it has accumulated on the ground.
-
Radioactive particles emit penetrating radiation that cause
radiation exposure that can
injure people (even in cars or within
poorly insulated shelters).
- Gamma rays in fallout are photons emitted by radionuclides.
- Like x-rays from machines, gamma rays from radionuclides can “shine” through (penetrate) clothing, walls, protective suits, cars, and inadequate shelters.
-
Radionuclides in fallout
-
Unlike releases from nuclear power plant accidents, the
majority of fission products released from a nuclear
detonation tend to be short lived.
See Figure 1 below.
- Radionuclides with short half-lives will dominate the exposure in the first few seconds, but then decay away.
-
Early radionuclides after a nuclear detonation:
seconds, minutes, hours
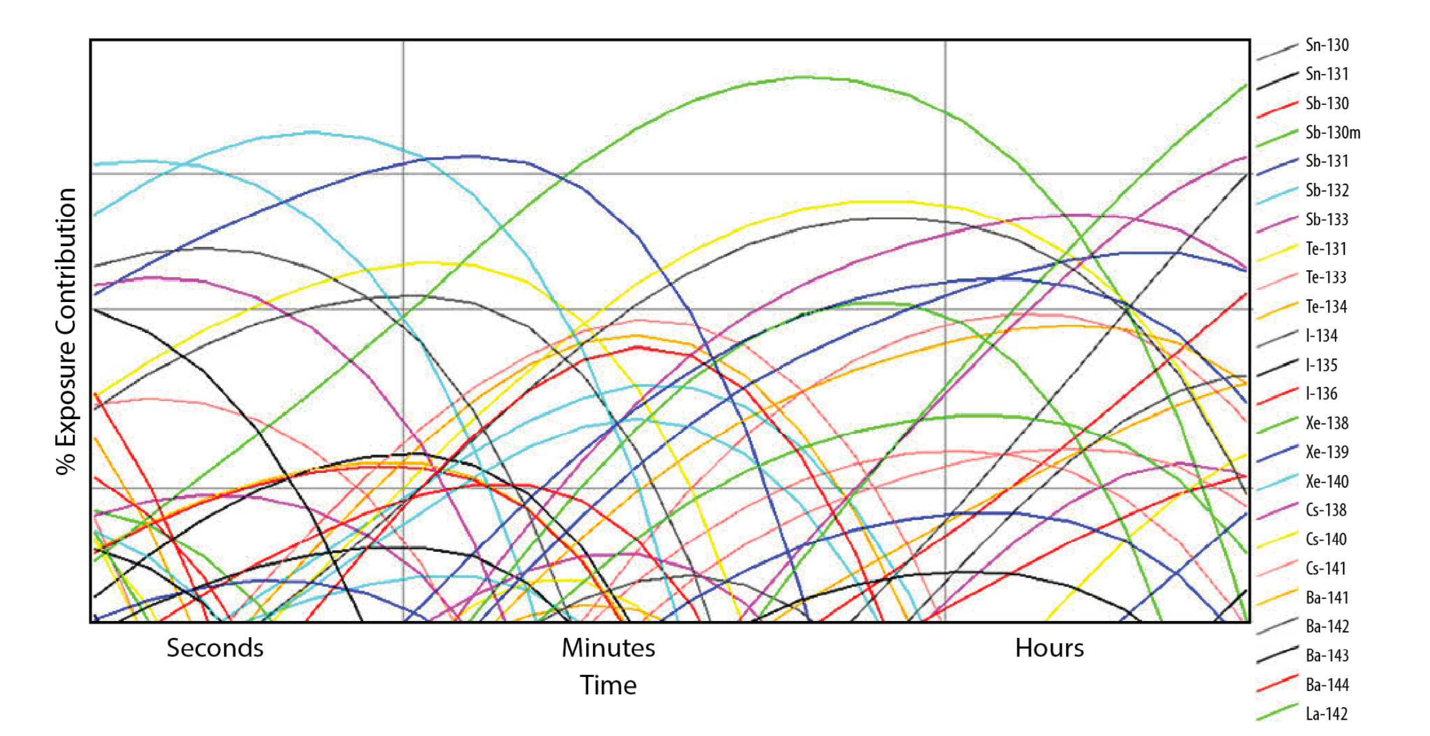
Figure 1. Examples of how nuclear fission product radionuclides change over time. Each line represents the growth and decay of a different radionuclide, a few of which are displayed in the legend.
-
Late radionuclides after a nuclear detonation: 100
days, 1 year, 10 years
Table 1 below provides some examples at specific times of the primary fallout activity contributors. Radionuclides that contribute less than 1% were not included.
Table 1: Primary Fallout Activity Contribution at 3 Different Times
Although the dangerous radiation levels will subside rapidly over the first few days, residual radiation from the long half-life fission products (such as 90Sr, 106Ru, 137Cs, 147Pm, and 155Eu) will become the main contributions to exposure (after about 10 years).Isotope Half Life Activity % @ 100 days Activity % @ 1 year Activity % @ 10 years Sr-89 50 d 11% 3% Sr-90 29 y 0.2% 3% 36% Y-91 59 d 22% 7% Zr-95 66 d 19% 2% Ru-103 40 d 19% 2% Ru-106 369 d 3% 24% 0.5% Cs-137 30 y 0.3% 3% 46% Ce-141 33 d 14% 0.7% Ce-144 284 d 8% 34% 0.2% Pm-147 2.6 y 1.4% 13% 14%
-
Rate of Decay of the dose rate from radiation from
fallout
(from the time of the explosion, not from the time of
fallout deposition).
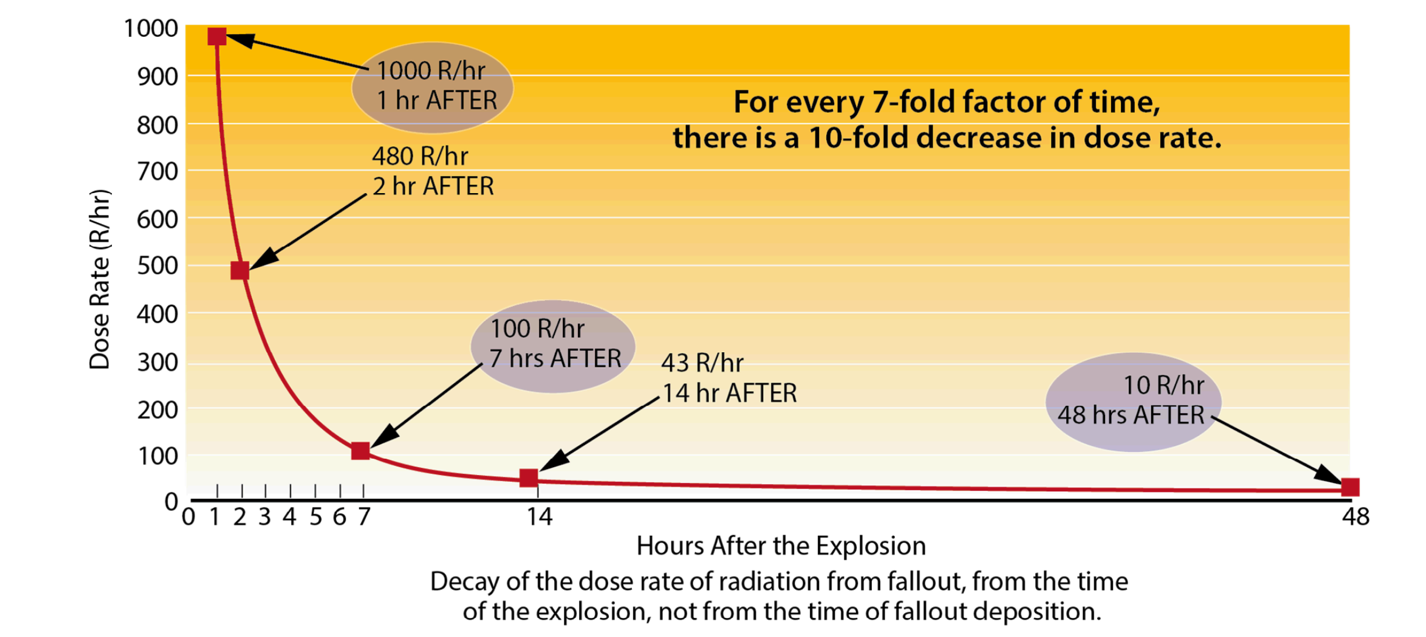
Figure 2. Decay of the dose rate of radiation from fallout (from the time of the explosion, not from the time of fallout deposition).- Note that the x-axis represents hours not days.
- For this example, an arbitrary 1-hour starting value of 1,000 R/hr (R = roentgen) was used.
- Because of the large amount of short-lived fission products, the activity and the radiation levels decrease rapidly with time.
- Fallout gives off more than 50% of its energy in the first hour and continues to decay rapidly even after that initial hour.
- Because radionuclides decay in the hours and days after detonation, the level of environmental radiation changes quickly over time, which is what influences the early shelter-in-place recommendations and location of venues for response activities.
-
Unlike releases from nuclear power plant accidents, the
majority of fission products released from a nuclear
detonation tend to be short lived.
See Figure 1 below.
External Exposure vs. Internal Exposure (Internal Contamination)
- Once fallout particles reach the ground, the most serious medical hazard arises from external exposure to penetrating radiation released from the decaying particles (gamma rays), rather than from breathing or ingestion of these radioactive particles.
-
External exposure
occurs when the source of the radiation is outside the body.
- This can include exposure from a point source, ground contamination, a passing cloud of radioactive material, or even contamination on the outside of the body.
- A person’s dose from exposure is determined by the amount of radiation energy absorbed by the body.
-
Stopping the external exposure will occur by
- Removing a person from the radioactive environment
- Removing (e.g., brushing off) the contamination from the clothing or skin
- Removing the contaminated clothing and changing into uncontaminated clothes.
-
Internal contamination (internal exposure)
- Occurs when radioactive material gets inside the body from either inhalation, ingestion, absorption through the skin, or absorption at the site of a wound.
-
Internal contamination (exposure) from nuclear
detonation fallout is not a primary clinical concern
during the early, emergency phase of the
response.
This is due to several important factors:
- Early fallout particles tend to be large particles (salt and sand sized), which are not easily inhaled into the lungs.
- The rapid, early decay of fallout means that any particles taken into the body do not generate long term exposures.
-
As a relative hazard, internal exposures are
generally orders of magnitude below external
exposures, as noted in the 3 documents below about
ground bursts.
-
Levanon I, Pernick A. The inhalation hazard of radioactive
fallout. Health Phys. 1988 Jun;54(6):645-57. [PubMed
Citation]
- Inhalation of fallout particles does NOT present a significant radiological hazard from a ground burst in the 0.5 kT to 10 mT yield range.
-
Peterson KR, Shapiro CS. Internal dose following a major nuclear
war. Health Phys. 1992 Jan;62(1):29-40. [PubMed
Citation]
- After sheltering in place at home or the workplace, the dose from external exposure was much higher and more significant clinically over time than the total internal dose from ingestion of the 4 most important radioisotopes.
-
Raine DA, Millage K, McClellan GE
(ARA-TR-09-SEASSP-17176-010, as cited in this
document)
- Provides guidance on the relative importance of internal doses from the inhalation and ingestion of fallout compared to external doses and blast and prompt radiation effects from a 10-kT nuclear detonation.
- Based on a scenario that assumes a person remains in the path of the descending fallout until it ends and using a mean particle size distribution that individually maximizes the dose from each radionuclide species, the total 50-year CEDEs from the inhalation of fallout are all less than 2.0 rem.
-
Levanon I, Pernick A. The inhalation hazard of radioactive
fallout. Health Phys. 1988 Jun;54(6):645-57. [PubMed
Citation]
Low Dose Rate in “Detectable Contamination” Areas at 24 hours post Nuclear Detonation
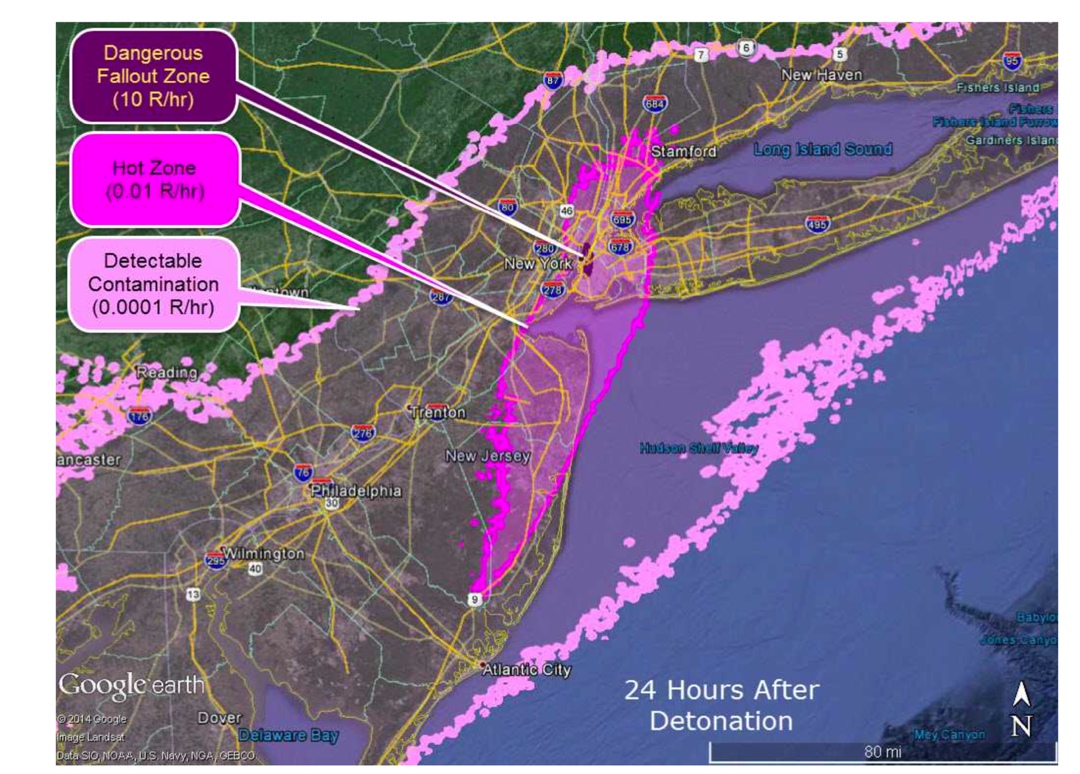
Figure 3. Low Dose Rate in “Detectable Contamination” Areas at 24 hours post Nuclear Detonation
- The graphic above is a computer-generated map of potential areas of contamination 24 hours after a hypothetical 10 kT nuclear detonation.
-
Note the 3 levels of ambient radiation: Dangerous Fallout
Zone, Hot Zone, and Detectable Contamination.
- “Detectable Contamination” here means 0.0001 R/hr, which is only 2–4 times normal background levels in the region, a very low level.
- Over time, the outer limits of each zone will change as radioactivity decays. See REMM page for more about marked time changes in the perimeter of the Dangerous Fallout Zone and Hot Zone.
- Handheld radiation survey equipment can measure radiation at these very low levels in the “Detectable Contamination” zone, even though these levels are far below any immediate health threat.
-
To be effective and reassuring, communicating with the
public about low level “Detectable
Contamination” requires careful public messaging, as
the public perceives any radiation is significantly
hazardous. See
Improvised Nuclear Device Response and Recovery:
Communicating in the Immediate Aftermath (US Government Interagency Nuclear Detonation
Response Communications Working Group, June 2013). This
information about low risk in the “Detectable
Contamination” areas needs to be communicated quickly
and accurately to the general public.
- It should help allay fears about personal risk and perception about the potential the need for urgent decontamination.
- Formal radiation monitoring is not required in these very low level “Detectable Contamination” areas, but self-decontamination should be encouraged, as feasible.
- Formal population decontamination venues, when established at later times in more distant sites, can be stand-alone or co-located with reception centers or transportation hubs and should focused on those who left (or traveled through) the “Dangerous Fallout Zone”.
- If population monitoring is performed in venues with large numbers of people in areas whose only exposure has been in areas with “Detectable Contamination” areas, response workers should rapidly scan members of the public for any immediately evident increased radiation (< 30 seconds per person).
- For very large numbers of evacuees undergoing scanning, scan just hands and feet. See Decision Levels.
Population Monitoring and Decontamination
Early Phase of the Incident
-
Because the radiation energy given off by
fallout particles decays rapidly with time, early gross, self-decontaminated (e.g., by brushing
contamination off clothes and skin for example) is better
than delaying decontamination to wait for formal
decontamination teams with radiation detection survey meters
to document the level of contamination, provide showering
facilities, and new clothes.
- Self-decontamination instructions can be found in Improvised Nuclear Device Response and Recovery: Communicating in the Immediate Aftermath (US Government Interagency Nuclear Detonation Response Communications Working Group, June 2013).
- See this REMM page about Decision Levels.
- Limited response resources (e.g., radiation survey meters, personnel, venues) should not be used for high volume population monitoring and decontamination operations in the first few days. Self-decontamination is preferred.
-
Formal decontamination venues, when established at later
times in more distant sites, can be stand-alone or
co-located with reception centers or transportation hubs and
should focus on those who left (or traveled through) the
Dangerous Fallout Zone.
- Consider placement of these centers near sources of replacement footwear and clothing.
- If additional decontamination is required beyond self-decontamination, efforts should focus on removing or replacing shoes and outer clothing and washing or wiping exposed skin and hair (which is why access to quantities of clothing is an important location consideration, especially in winter).
Intermediate Phase of an Incident
- As shown in fallout contamination decays rapidly (giving off > 80% of its energy in the first day) so early, gross decontamination (such as removing/changing outer layer of clothing) is far more effective than a delayed, if more thorough, wash down.
- As the event progresses past the first few days, the fallout decay rate will slow and there may be more resources (stuff, staff, space) and time for more formal radiation monitoring and decontamination.
Population Monitoring and Decontamination
- Population monitoring is defined by the CDC as the tasks required to “identify, screen, measure and monitor populations (people and their pets) for exposure to radiation or contamination from radioactive materials”.
- In the aftermath of a large-scale radiation release, there will be a need to assess large groups of individuals and prioritize their care from immediate urgent medical needs to potential long-term effects resulting from the radiation incident.
- As always, life-threatening medical issues take priority over radiation detection and decontamination issues.
-
Because the needs of large populations need to be addressed
and radioisotopes decay quickly, a plan for
self- decontamination for most people can
provide many benefits (faster, applicable to large
populations quickly), as discussed in the monographs below
- Responding to a Radiological or Nuclear Terrorism Incident: A Guide for Decision Makers (PDF - 1.61 MB) (NCRP Report No. 165), Bethesda, MD, 2010.
- Population Monitoring and Radionuclide Decorporation Following a Radiological or Nuclear Incident, (NCRP Report No. 166), Bethesda, MD, 2011.
- Population Monitoring in Radiation Emergencies, A Guide for State and Local Public Health Planners, Second Edition, (PDF - 13 MB) (HHS/CDC, April 2014)
- Formal decontamination venues, when established at later times in more distant sites, can be stand-alone or co-located with reception centers or transportation hubs and should focus on those who left (or traveled through) the Dangerous Fallout Zone.
- If and when formal radiation detection procedures are implemented for screening, decisions need to be made about what levels will trigger formal decontamination and when is it acceptable to stop decontamination (See Decision Levels on this page, and REMM page about Target Levels for Decontamination).
- Good radiation survey assessments must incorporate the instrument’s capabilities and limits, and the method used (survey technique) that is appropriate. See REMM page about radiation surveys.
- Regardless of the approach utilized for large populations (self-decontamination or formal surveys and decontamination), it will be important to pair it with public messaging about risk and personal actions that provides clear instructions and helps to reduce the stress that comes with incidents.
- Survey procedures selected will likely require consultation with the US government Advisory Team for Environment, Food and Health will likely be required
- See REMM page about How to Perform a Radiation Survey
Decision Levels: Benchmarks—when to start and when to stop
- During the early phase of an incident, when resources are scarce, self-decontamination is likely to be the predominant recommendation.
- “Decision Levels” (for when formal decontamination is needed and when it can stop) are not universally agreed upon.
- The biggest influences on what is recommended are how many people need services, risks on the ground, the survey instruments used and how the detection is performed.
- An excellent, comprehensive review of Population Monitoring and of Decision Levels is available in the ROSS Toolkit. This is found on the RadResponder.net web site which requires access privileges and login. After login, see ROSS Toolkit > Resources > Population Monitoring
Key Points from Two Other Important Documents
-
Population Monitoring in Radiation Emergencies: A Guide for State and Local Public Health Planners, Second Edition, 2014 (PDF - 13 MB) (HHS/CDC)
-
The first priority is to save lives: respond to and
treat the injured first.
- Treatment of life- or limb-threatening medical conditions should take precedence over radiation decontamination.
- Standard Precautions are generally adequate to provide protection for first responders, emergency medical personnel, and clinicians.
-
Contamination with radioactive materials is not
immediately life-threatening.
- Decontamination procedures are straightforward.
- Removing clothing and washing the body thoroughly with mild soap and water will eliminate most external contamination.
-
Initial population monitoring activities should focus
on preventing acute radiation health effects from
exposure not contamination
- Cross-contamination issues are a secondary concern, especially when the contaminated area or the affected population is large.
-
Scalability and flexibility are important parts of
the planning process.
- The standard criteria used for contamination screening and the radiation survey methods may have to be adjusted to accommodate the magnitude of the incident and availability of resources.
-
Fear of radiation is high, perhaps higher than with
other agents of terrorism.
- Providing information and clear communication prior to and during an incident will help allay fears and allow people to make appropriate response decisions.
-
A key resource for implementing activities described
in this guide is a state’s lead agency for
radiation control.
- Additional expertise and resources to plan for and respond to a radiation incident can be obtained from radiation protection professionals in each community.
- Local emergency response plans should identify experts such as health physicists or radiation safety officers in area health departments, environmental agencies, hospitals, and universities.
- Relationships with these experts should be established in the planning stages.
-
First responders and local officials may not be aware
initially that a radiation incident has
occurred.
- Public health and emergency personnel’s initial response to an incident may be an all- hazards approach.
- However, once these personnel have determined that radiation or radioactive material is involved, they must begin addressing the issues related to this type of incident.
-
Decontamination should be done as soon as possible,
but it usually does not require the same immediacy as
chemical or biological contamination does.
- Radiological decontamination recommendations differ from those for chemical or biological agents.
- Decontamination for chemical or biological agents must be performed immediately.
- In a radiation emergency, people may be advised to self-decontaminate at home or at a community reception center.
- Law enforcement agencies will be involved in response to a radiological terrorism incident.
-
If a radiation incident is the result of a terrorist
attack, the site will be considered a crime
scene.
- Close coordination with local, state, tribal, and federal law enforcement agencies will be required to manage the public health response, because both public health and law enforcement personnel will need to conduct operations in the same area.
-
The first priority is to save lives: respond to and
treat the injured first.
-
National Planning Guidance for Response to a Nuclear Detonation, Second Edition (PDF - 2.69 MB) (USG Interagency, 2010)
Radioactive contamination is not immediately life threatening.
- Identification of individuals whose health is in immediate danger and require urgent care is the immediate priority of any population monitoring activity. Near the incident scene, this monitoring need is accomplished as part of the medical triage already described in Chapter 4. Management of serious injury takes precedence over radiological decontamination.
- The primary purpose of population monitoring, following a nuclear detonation, is detection and removal of external contamination. In most cases external decontamination can be self- performed, if straightforward instructions are provided. There are two types of decontamination. External decontamination removes fallout particles and other radioactive debris from clothes and external surface of the body. Internal decontamination, if needed, requires medical treatment to reduce the amount of radioactivity in the body.
- Prevention of acute radiation health effects should be the primary concern when monitoring for radioactive contamination. Population monitoring personnel should offer or recommend gross external decontamination such as brushing away dust or removal of outer clothing. Cross-contamination issues (e.g., from transport vehicles) are of secondary concern, especially in a nuclear emergency where the contaminated area and the potentially impacted population are large.
- Population monitoring and decontamination activities should remain flexible and scalable to reflect the available resources and competing priorities. For example, if water is a scarce commodity or is needed to fight fires, dry methods can be used for decontamination. Moist wipes can be used to wipe the face and hands in addition to a change of outer clothing. Instead of pouring water as in a shower, small amounts of water can be used to wet paper towels and clean the skin.
- Radioactive contamination is not immediately life threatening. Individuals who are self- evacuating may be advised to self-decontaminate. Suggestions for monitoring and decontamination in this chapter assume radioactivity is the only contaminant and that there are no chemical or contagious biological agents present.
Key Quotes from Other Important Documents
-
“Skin or wound contamination is
never immediately life threatening to
affected people or medical personnel.”
Protecting People against Radiation Exposure in the Event of a Radiological Attack, (International Commission on Radiological Protection, Publication No. 96)
-
“..rescue and medical emergencies take precedence over
radiological concerns.”
Key Elements of Preparing Emergency Responders for Nuclear and Radiological Terrorism, NCRP Commentary No. 19, 2005)
-
“..Radioactive material contamination rarely
represents an Immediate danger to the health of the victim
or the responder. This reduces the immediacy of the need for
decontamination and allows the emergency response community
greater flexibility in selecting decontamination
options.”
Key Elements of Preparing Emergency Responders for Nuclear and Radiological Terrorism, NCRP Commentary No. 19, 2005)
-
“The initial screening criteria must focus on
preventing acute health effects and must take into account
the magnitude of the incident and availability of
resources.”
Population Monitoring in Radiation Emergencies: A Guide for State and Local Public Health Planners, Second Edition, 2014, (HHS/CDC)